
Quick Answer: Kidney stones form when your urine contains more crystal-forming substances such as calcium, oxalate, and uric acid than the fluid in your urine can dilute. This chemical imbalance allows minerals to crystallize, clump together, and grow into hard masses within the renal pelvis or ureters.
The single most common driver of this process is chronic dehydration, which raises urinary concentration. Other key triggers include high-sodium diets, excessive animal protein, metabolic conditions like hypercalciuria, and genetic predispositions. To reverse this process, patients must systematically lower their urinary supersaturation levels through targeted fluid intake and dietary modifications.
1. Introduction to Nephrolithiasis: The Internal Crisis
Kidney stones, known clinically as nephrolithiasis or renal calculi, represent one of the most painful and complex metabolic disorders of the urinary tract. In the clinical setting, we do not view a kidney stone as an isolated event. Instead, it is the crystalline endpoint of a systemic, multi-faceted metabolic imbalance.
When a patient presents to the clinic with acute, radiating flank pain, they are dealing with a structural blockage. However, the root problem is biochemical. Understanding what causes kidney stones requires a deep dive into how our bodies process minerals, handle hydration, and regulate urinary pH.
To contextualize where and how these stones develop, it is helpful to look at the internal anatomy of the renal system:
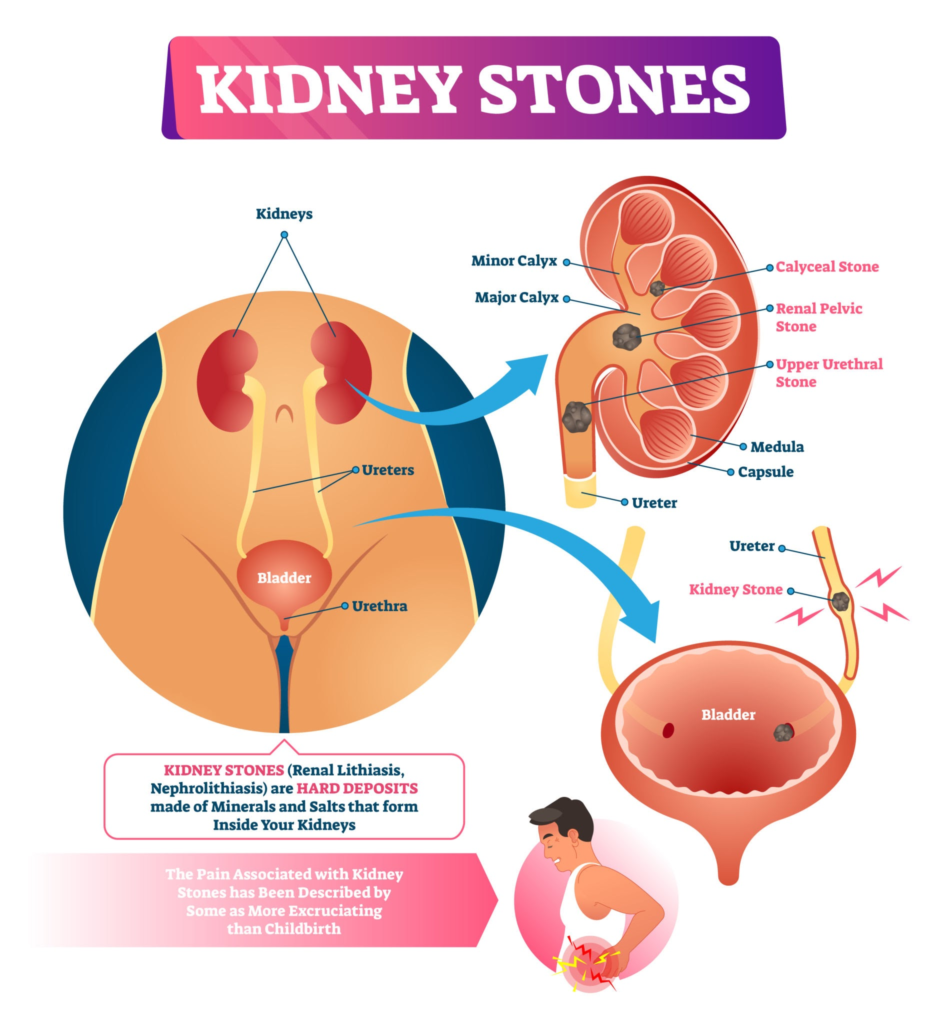
As shown above, stones can form within the minor and major calyces, the renal pelvis, or migrate downward into the narrow ureter, causing severe obstruction. By understanding the underlying mechanics of causes of kidney stones, we can move past simple symptom management and focus on true preventative care.
2. The Core Physics and Biochemistry of Stone Formation
At its most fundamental level, stone formation relies on a physical chemistry principle called supersaturation.
The Saturation Continuum
Your urine is a highly complex solution containing dissolved salts, minerals, and organic waste compounds. Under normal physiological conditions, these elements remain perfectly dissolved. However, if the balance shifts, the solution moves through three distinct zones:
- Undersaturated Zone: Mineral concentrations are low. Existing stones dissolve, and new crystals cannot form.
- Metastable Zone: The urine holds more minerals than a simple water solution could, but natural urinary inhibitors (such as citrate and magnesium) keep them from clumping. However, if a solid “seed” crystal is introduced, growth can occur.
- Supersaturated Zone: The mineral concentration exceeds the urine’s holding capacity. Spontaneous crystallization becomes inevitable.
Nucleation, Growth, and Aggregation
Once urine enters the supersaturated state, the formation process follows a strict thermodynamic sequence:
- Nucleation: The initial step where microscopic ion clusters (like calcium and oxalate) bond together to form a solid nucleus. This often occurs on an anatomical landing pad known as Randall’s Plaques—microscopic patches of calcium phosphate on the renal papillae that act as an anchor.
- Crystal Growth: Solute molecules continually attach themselves to the newly formed nucleus, increasing its physical dimensions.
- Aggregation: Multiple distinct crystals collide and fuse together, forming a larger mass. This is the exact moment a microscopic crystal transitions into a clinically significant, sharp-edged macroscopic stone capable of scraping the delicate epithelial lining of the urinary tract.
3. The 4 Major Types of Kidney Stones and Their Triggers
Not all renal stones are chemically identical. Effectively preventing a recurrence requires knowing exactly what your stone is made of.
+—————————————————————————–+
| KIDNEY STONE TYPES |
+—————————————————————————–+
| |
| [ Calcium Oxalate / Phosphate ] (75-80%) |
| ├── Driven by: Dehydration, High Sodium, Hypercalciuria |
| └── Appearance: Sharp, jagged, dark brown/amber |
| |
| [ Uric Acid Stones ] (5-10%) |
| ├── Driven by: Low Urinary pH (<5.5), High Purine Diets, Gout |
| └── Appearance: Smooth, round, reddish-orange |
| |
| [ Struvite / Infection Stones ] (10-15%) |
| ├── Driven by: Urease-producing UTIs (Proteus, Klebsiella) |
| └── Appearance: Staghorn formations filling the renal pelvis |
| |
| [ Cystine Stones ] (<1%) |
| ├── Driven by: Autosomal Recessive Genetic Defect (SLC3A1/SLC7A9 genes) |
| └── Appearance: Smooth, yellow, waxy crystalline structures |
| |
+—————————————————————————–+
Calcium Oxalate and Calcium Phosphate (75% to 80% of Cases)
This is the most common variety. These stones form when calcium binds with oxalate or phosphate in highly concentrated urine. This process is frequently accelerated by hypercalciuria (excess calcium in the urine), hypocitraturia (insufficient citrate, which is a natural stone inhibitor), and elevated dietary sodium, which forces the kidneys to dump more calcium into the urine.
Uric Acid Stones (5% to 10% of Cases)
Uric acid is a byproduct of purine metabolism. These stones are distinct because they do not require high levels of uric acid to form; instead, their primary driver is a persistently low urinary pH (acidic urine, below 5.5). In an acidic environment, uric acid becomes highly insoluble. This issue is common in patients with high animal protein diets, metabolic syndrome, type 2 diabetes, or gout.
Struvite Stones (10% to 15% of Cases)
Also known as infection stones, these are composed of magnesium ammonium phosphate. They form almost exclusively in response to chronic upper urinary tract infections caused by urease-producing bacteria (such as Proteus mirabilis or Klebsiella pneumoniae). These bacteria split urea in the urine to create ammonia, rapidly raising the urinary pH to an abnormally alkaline level (above 7.2) and creating the perfect environment for massive staghorn stones to fill the renal calyces.
Cystine Stones (Less than 1% of Cases)
These rare stones are caused by an inherited autosomal recessive genetic defect. The mutations affect the SLC3A1 and SLC7A9 genes, which code for the renal amino acid transporter responsible for reabsorbing cystine, ornithine, lysine, and arginine. When this transporter fails, huge amounts of insoluble cystine spill into the urine, crystallizing into smooth, yellow, waxy stones that often appear early in childhood.
4. Unmasking the Roots: Historical and Metabolic Triggers
To fully understand why these crystal imbalances occur, we have to look back at the historical evolution of the condition, alongside the persistent physiological reasons why some individuals suffer from chronic recurrences.
The Historical Context: Evolutionary Adaptations vs. Modern Lifestyles
When exploring the deep kidney stones origins, historical and anthropological records show that nephrolithiasis was once a relatively rare metabolic issue, often restricted to the wealthy who had access to heavy meats and alcohol. Today, it has transformed into a widespread global health issue affecting over 10% of the population.
This dramatic shift is primarily a mismatch between our evolutionary biology and modern lifestyles. Our ancestors evolved complex mechanisms to conserve sodium and concentrated urine to survive periods of intense heat and scarce water. In today’s landscape of processed foods, hidden dietary sodium, and chronic low-grade dehydration from desk-bound environments, these ancient survival mechanisms end up backfiring, turning our kidneys into crystal-producing environments.
The Cycle of Recurrence: Why Stones Keep Coming Back
A common question in nephrology clinics is: why do people get kidney stones again and again? The answer lies in unaddressed systemic metabolic defects.
If a patient receives treatment for a stone but never changes the underlying biochemistry of their urine, their risk of a five-year recurrence sits at roughly 50%. The primary reasons for this cycle include:
- Persistent Idiopathic Hypercalciuria: A genetic trait where the intestines absorb too much calcium, or the renal tubules fail to reabsorb it, causing high levels of calcium to constantly spill into the urine regardless of dietary intake.
- Uncorrected Hypocitraturia: Citrate is the body’s primary defense against stones; it binds to urinary calcium to form a highly soluble compound, effectively preventing calcium from binding with oxalate. Chronic systemic acidity, often caused by heavy animal protein diets, uses up citrate during the body’s internal buffering process, leaving the urine unprotected.
- Unchanged Structural Microenvironments: Once a stone forms and damages the renal papillae, it can leave behind scarred tissue and persistent microscopic calcium deposits (Randall’s plaques) that serve as permanent foundations for future crystal growth.
5. Debunking the Myth Engine: Beverages and Dietary Misconceptions
One of the largest hurdles in preventative nephrology is clearing up misinformation. Patients are often bombarded with conflicting advice regarding which drinks cause or prevent stones. Let’s break down the actual clinical evidence behind common beverage myths.
The Gatorade Debate
Many athletes and manual laborers wonder: does gatorade cause kidney stones? The truth requires a balanced view of electrolytes.
While sports drinks do provide hydration, they also contain significant amounts of added sodium and refined sugars. High sodium intake forces your kidneys to excrete more calcium into your urine, while refined sugars can spike urinary calcium levels and reduce urine volume.
Therefore, relying purely on commercial sports drinks for daily hydration is counterproductive. For a detailed clinical breakdown of how sports drinks affect mineral excretion, review our comprehensive analysis on the kidney stones causes prevention gatorade truth.
The Danger of Energy Drinks
In contrast to the nuanced view of sports drinks, the connection between energy drinks and renal issues is much clearer. So, do energy drinks cause kidney stones? Yes, they are significant risk factors.
Energy drinks typically carry massive doses of caffeine, which acts as a renal diuretic. This accelerates fluid loss and increases urinary calcium excretion. Additionally, many of these drinks are loaded with high-fructose corn syrup, which alters urinary pH and elevates uric acid production, alongside excessive synthetic vitamins that can overtax renal filtration.
Hard Water vs. Soft Water
A very frequent question from patients is whether tap water quality affects stone formation: does hard water cause kidney stones?
Logically, people assume that because hard water contains high levels of calcium and magnesium, it must increase stone risk. However, extensive epidemiological studies show no direct link between drinking hard water and an increased incidence of kidney stones.
In fact, the calcium and magnesium found in hard water can actually bind to dietary oxalate within your digestive tract, preventing it from being absorbed into your bloodstream and spilling into your kidneys.
The Citrus Family: Grapefruit Juice vs. Lemon Juice
The impact of citrus fruits on stone formation varies significantly by fruit type. For example, does grapefruit juice cause kidney stones? Clinical data suggests it might.
Large prospective cohort studies have found a correlation between regular grapefruit juice consumption and an increased risk of stone formation. The exact mechanism is still being studied, but it is believed that specific compounds in grapefruit juice can alter the enzymatic breakdown of organic acids, potentially increasing urinary oxalate excretion.
This stands in stark contrast to lemon juice, which is rich in citric acid and helps prevent stones by raising urinary citrate levels.
Alcohol, Soda, and General Hydration
When managing stone risk, you must evaluate everything you drink. Let’s look at the broader landscape of kidney stones and beverages to see how different options alter your urinary chemistry:
- Dark Sodas (Colas): High risk. These are preserved using phosphoric acid, which directly acidifies urine and pulls calcium out of bones into the kidneys.
- Is There an Alcohol Connection? To understand if is there a connection between alcohol and kidney stones, you have to look at fluid balance. Alcohol inhibits anti-diuretic hormone (ADH), leading to rapid dehydration and highly concentrated urine. While moderate beer consumption provides a short-term diuretic effect that may help clear microscopic crystals, the subsequent dehydration risk and purine load from heavier alcohol use significantly increase uric acid stone risks.
6. Real-Life Clinical Case Studies
To see how these metabolic factors interact in the real world, let’s examine two distinct patient profiles from clinical practice.
Case Study 1: The Dehydrated Office Worker
- Patient: 42-year-old male corporate executive.
- Presentation: Acute, agonizing left flank pain radiating to the groin, accompanied by nausea.
- Dietary History: Consumed 4–5 cups of black coffee daily, minimal plain water, high-sodium fast food lunches, and an energy drink every afternoon to beat the desk slump.
- Lab Findings: Non-contrast CT scan revealed a 4mm calcium oxalate stone in the left proximal ureter. Urinalysis showed a low urine volume (0.9 liters/day) and a highly acidic urinary pH of 5.2.
- Clinical Analysis: This patient’s stone was driven by chronic dehydration combined with high caffeine and sodium intake. The low urine volume caused extreme supersaturation, allowing calcium and oxalate to rapidly nucleate and grow.
- Intervention: The stone passed naturally with heavy hydration and alpha-blocker therapy. Long-term prevention focused on replacing energy drinks with mineral water, capping coffee at two cups daily, and keeping a 2.5-liter water bottle at his desk. He has remained stone-free for four years.
Case Study 2: The Well-Intentioned Health Enthusiast
- Patient: 35-year-old female fitness instructor.
- Presentation: History of three recurrent kidney stones over three years.
- Dietary History: To maintain a clean diet, she consumed a daily green smoothie packed with raw spinach, almond milk, and chia seeds. She also avoided dairy entirely, believing calcium was the root cause of her stones.
- Lab Findings: 24-hour urine collection revealed severe hyperoxaluria (urinary oxalate at 65 mg/day, normal is less than 40 mg/day) and very low urinary calcium.
- Clinical Analysis: By cutting out dairy, this patient eliminated the dietary calcium needed to bind oxalate in her gut. Meanwhile, her daily spinach and almond smoothies flooded her digestive tract with free oxalate, which was rapidly absorbed into her bloodstream and excreted by her kidneys, leading to recurrent stones.
- Intervention: She was instructed to swap high-oxalate spinach for low-oxalate kale, switch from almond milk to coconut milk, and ensure she consumed a source of calcium (like a lactose-free yogurt or calcium-citrate supplement) alongside her meals. Her urinary oxalate levels dropped back to normal, breaking her chronic recurrence cycle.
7. Deep-Dive Prevention Strategy: The 24-Hour Urine Blueprint
True stone prevention cannot rely on guesswork. The gold standard for building a preventative strategy is a 24-Hour Urine Collection Analysis. This diagnostic test measures the exact volume, pH, and mineral content of your urine over a full day.
Using the results of a 24-hour analysis, we can apply specific dietary changes to alter your urinary chemistry:
| Metric Evaluated | Target Clinical Range | Dietary/Lifestyle Action Required |
| Total Urine Volume | Greater than 2.5 Liters | Increase total fluid intake to 3–3.5 liters per day, spread evenly across waking hours. |
| Urinary Calcium | Less than 250 mg/day (M) / Less than 200 mg/day (F) | Do not reduce dietary calcium. Instead, drastically reduce sodium intake to under 2,000 mg/day to prevent the kidneys from wasting calcium. |
| Urinary Oxalate | Less than 40 mg/day | Limit high-oxalate foods (spinach, rhubarb, almonds, beets). Pair moderate oxalate foods with dietary calcium. |
| Urinary Citrate | Greater than 450 mg/day | Increase consumption of natural citrus elements (lemon or lime water) or introduce potassium citrate supplementation. |
| Urinary pH | Optimal: 6.2 – 6.8 | For uric acid stones (pH < 5.5), reduce animal protein and increase fruits and vegetables. For struvite/alkaline stones (pH > 7.2), treat underlying infections. |
8. Clinical Takeaways for Patient Care
When managing stone disease, keep these four essential clinical rules in mind:
- Hydration is About Volume, Not Just Effort: It does not matter how much water you think you are drinking; the only metric that matters is producing more than 2.5 liters of urine daily. If your urine is dark yellow, you are in the supersaturation danger zone.
- Never Starve Your Body of Calcium: Cutting calcium out of your diet to prevent calcium stones actually increases your risk. Dietary calcium is crucial because it binds with oxalate in your intestines, allowing it to be safely excreted through your stool rather than entering your kidneys.
- Sodium is the Hidden Enemy: High sodium intake pulls calcium out of your bones and dumps it straight into your urine. Reducing processed food intake is often more effective at lowering urinary calcium than changing your actual calcium consumption.
- Know Your Stone’s Chemistry: Treating a uric acid stone requires a completely different approach than treating a calcium phosphate or struvite stone. Always save passed stones for laboratory crystal analysis.
9. Comprehensive Myths vs. Medical Facts
To help you cut through the noise, let’s address the ten most common misconceptions about kidney stones with clear, evidence-based medical facts:
Myth 1: Cranberry juice cures all types of kidney stones.
- The Fact: Cranberry juice is highly acidic and contains moderate oxalate levels. While it can help prevent certain urinary tract infections, it can actually increase the risk of calcium oxalate stone formation by acidifying the urine and adding to the body’s oxalate load.
Myth 2: Kidney stones are always caused by a faulty diet.
- The Fact: While diet is a major component, genetics and metabolic conditions play a massive role. Inherited conditions like renal tubular acidosis, cystinuria, and primary hyperoxaluria can cause severe stone disease even in patients with perfect dietary habits.
Myth 3: If you pass a stone, the problem is completely solved.
- The Fact: Passing a stone simply removes the acute blockage. The underlying metabolic imbalance that created the stone remains. Without targeted lifestyle changes, the likelihood of forming another stone within five years is roughly 50%.
Myth 4: Olive oil and lemon juice mixtures can instantly dissolve large stones in the ureter.
- The Fact: No home remedy can instantly dissolve a stone lodged in the ureter. While lemon juice provides beneficial citrate that can help prevent future stone growth in the kidney, it cannot melt an existing solid crystalline mass during an acute attack.
Myth 5: Beer is an effective medical treatment for flushing out kidney stones.
- The Fact: Alcohol suppresses anti-diuretic hormone, which causes a short-term increase in urine output. However, this is quickly followed by severe rebound dehydration, which concentrates your urine and accelerates stone growth. Additionally, beer is rich in purines, which can trigger uric acid stones.
Myth 6: You can easily feel a kidney stone growing inside your kidney.
- The Fact: Stones sitting quietly within the renal pelvis are often completely asymptomatic and painless. The severe, agonizing pain only begins when the stone moves out of the kidney and becomes stuck in the narrow, muscular ureter, causing urine to back up and stretch the renal capsule.
Myth 7: All kidney stones require surgical intervention or laser treatments.
- The Fact: Most small stones (under 5mm in diameter) have an 80% to 90% chance of passing on their own with proper hydration, pain management, and medical therapies like alpha-blockers to relax the ureteral muscles.
Myth 8: Taking vitamin C supplements has zero effect on kidney stone risk.
- The Fact: High-dose vitamin C supplements (over 1,000 mg/day) can be dangerous for stone formers. The body breaks down excess vitamin C into oxalate, which significantly raises urinary oxalate levels and increases stone risk.
Myth 9: Drinking carbonated sparkling water causes kidney stones.
- The Fact: Plain sparkling water or seltzer does not cause stones. The carbonation process uses carbon dioxide, which does not alter urinary mineral concentration. However, avoid sparkling waters with added sodium or high-fructose corn syrup.
Myth 10: Kidney stones are a isolated issue that doesn’t impact long-term health.
- The Fact: Chronic, untreated kidney stones can lead to repeated urinary tract infections, progressive scarring of the renal tissue, and a gradual decline in overall kidney function, which can ultimately increase the risk of chronic kidney disease (CKD).
10. Frequently Asked Questions
Most stones under 5mm will pass on their own within one to four weeks. The exact timeline depends on the stone’s location, shape, and the patient’s fluid intake.
Chronic emotional stress elevates cortisol and aldosterone levels. These hormones can alter fluid balance, promote low-grade systemic inflammation, and increase the excretion of minerals like calcium into the urine, indirectly raising your stone risk.
Urine production naturally slows down and concentrates while you sleep, causing the kidneys to contract more forcefully against any existing blockages. Additionally, people move around less at night, which can cause a stone to settle into a painful position within the ureter.
Yes, hyperparathyroidism—a condition where the parathyroid glands produce too much parathyroid hormone (PTH)—causes bones to release excess calcium into the bloodstream. This leads to high blood calcium levels (hypercalcemia) and a significant increase in urinary calcium, resulting in recurrent stone formation.
Yes, it is possible. As a stone moves or shifts within the kidney’s collecting system, its sharp edges can scrape the delicate lining of the urinary tract, causing microscopic or visible blood to spill into the urine even before a painful blockage occurs.
11. References and Citations
- Pearle, M. S., & Goldfarb, D. S. (2014). Medical Management of Kidney Stones: AUA Guideline. Journal of Urology, 192(2), 316-324.
- Coe, F. L., Evan, A., & Worcester, P. (2005). Kidney stone disease. The Journal of Clinical Investigation, 115(10), 2598-2608.
- Curhan, G. C., Willett, W. C., Rimm, E. B., & Stampfer, M. J. (1993). A prospective study of dietary calcium and other nutrients and the risk of symptomatic kidney stones. New England Journal of Medicine, 328(12), 833-838.
- Scales, C. D., Smith, A. C., Hanley, J. M., & Saigal, C. S. (2012). Prevalence of kidney stones in the United States. European Urology, 62(1), 160-165.
Medical Disclaimer
The information provided in this article is for educational and informational purposes only. It is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or a qualified nephrologist/urologist with any questions you may have regarding a medical condition or treatment plan.
Author Profile
Dr. Adam N. Khan, MD
Dr. Adam N. Khan is a board-certified Nephrologist and Medical Reviewer with over 15 years of clinical experience diagnosing and managing complex metabolic kidney disorders, chronic kidney disease (CKD), and recurrent nephrolithiasis. He completed his medical training and fellowship in nephrology at top-tier university medical centers and currently serves as a clinical consultant, helping patients manage their kidney health through evidence-based dietary interventions and advanced medical therapies.
Renal Diet Recipes: Easy Breakfast, Lunch & Dinner Ideas
Acute Kidney Injury Guide: Causes, Stages, and Recovery
Natural Supplements for Kidney Health: Science-Backed Guide
Kidney Stone Size and Treatment Guide: Chart, Sizes & Surgery
Chronic Kidney Disease Stages: Complete 1 to 5 Clinical Guide
Early Warning Signs of Kidney Disease: Symptoms & Failure Guide
Renal Diet Plan: The Complete Kidney-Friendly Meal Guide