
By Dr. Adam N. Khan, MD, FAAFP
Medically reviewed by Dr. Adam N. Khan, MD, Infectious Disease Specialist
It was a Tuesday morning, and Eleanor Vance sat across from me in exam room 4, looking exhausted and a little lost. She’s 68, a retired librarian, sharp as a tack normally, the kind of person who brings me a neatly typed list of her concerns. That day, she had no list. She just slumped in the chair and said, “I don’t know what’s wrong with me, doc. I can’t eat. My stomach hurts all the time. I feel like I’m ninety.” Her daughter, sitting quietly in the corner, mouthed “she’s been so confused.”
Eleanor told me she’d been feeling “off” for weeks. Nausea that wouldn’t quit. A bone-deep fatigue that wasn’t like regular tiredness — this was the kind that made walking from the bedroom to the kitchen feel like a climb. She was constipated no matter what she ate. She was thirsty. All. The. Time. She’d get up four, five times a night to pee, which only made the exhaustion worse. And her muscles ached; she blamed it on gardening but it wasn’t muscle soreness, it was a dull, creeping pain that wouldn’t let go.
When I asked about medications and supplements, her daughter pulled out a bottle. High‑dose vitamin D3 — 10,000 IU per capsule — and a calcium supplement, 600 mg twice a day. Eleanor had been taking them faithfully for almost a year after a friend told her they would “protect her bones” and “boost her immunity” during the pandemic. No one had ever checked her vitamin D level.
The labs I ordered that morning told the story. Her serum calcium was 12.8 mg/dL (normal is around 8.6–10.3). Her creatinine, a marker of kidney function, had jumped to 1.9 from 0.9 just a year earlier — an acute kidney injury. Her 25‑hydroxyvitamin D level, the storage form, came back at 148 ng/mL. Anything above 100 ng/mL is considered toxic. Eleanor’s kidneys were paying the price for a well‑intentioned supplement that had quietly, silently, climbed into dangerous territory.
I sat back down, pulled my stool close, and told her plainly: “Your kidneys are angry because there’s too much calcium in your blood, and that came from too much vitamin D. We need to stop everything now and fix this.”
She looked at me with a mix of fear and relief — finally knowing what it was. That moment is exactly why I want to walk you through everything you need to know about vitamin D and your kidneys, from what it feels like when things go wrong to exactly how we fix it, and how to protect yourself from it ever happening.
So How Does Vitamin D Actually Affect the Kidneys?
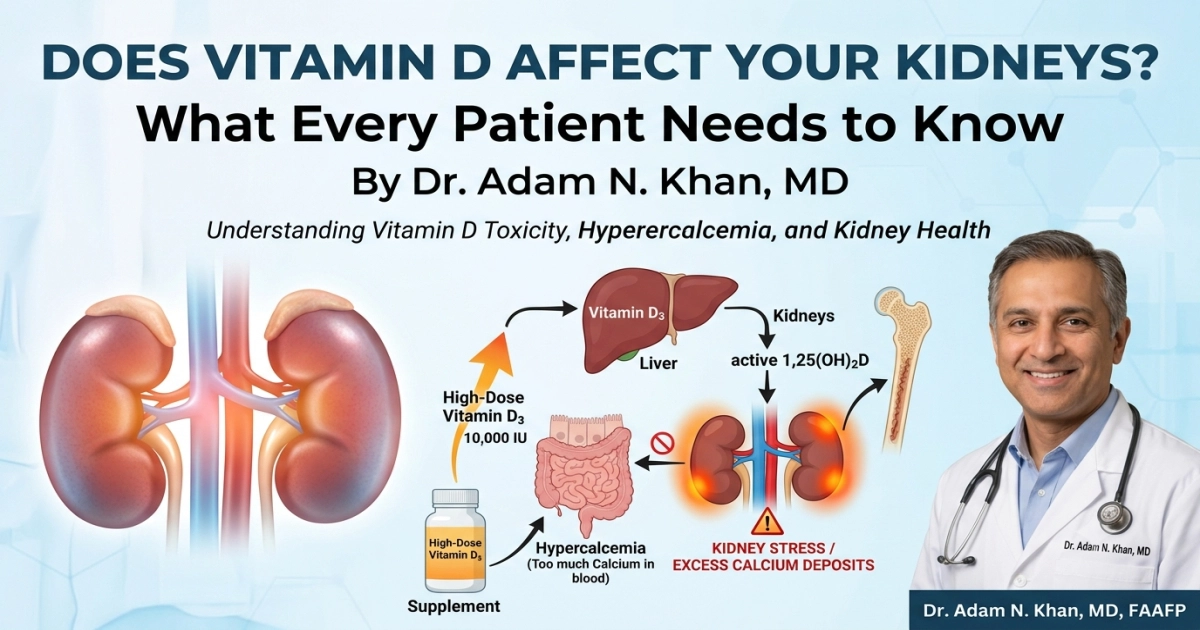
Here’s the part most people don’t realize: your kidneys and vitamin D are in a lifelong partnership. The vitamin D you swallow — whether from a pill or from sun‑exposed skin — is biologically inert. It travels to the liver, gets a chemical tweak, and becomes 25‑hydroxyvitamin D (the form we measure in blood tests). But the final, most powerful activation? That happens in your kidneys. A special enzyme there converts it into 1,25‑dihydroxyvitamin D, or calcitriol, which then goes on to tightly regulate calcium and phosphorus in your body, keep your bones strong, and modulate your immune system.
When the kidneys are healthy, this whole system runs like a quiet orchestra. When you take too much vitamin D, the orchestra goes haywire. Excess vitamin D tells your gut to absorb way too much calcium from your food and supplements. The calcium spills into your bloodstream. That leads to hypercalcemia — too much calcium in the blood — which directly constricts the blood vessels inside your kidneys, triggers massive dehydration from constant urination, and can cause calcium to deposit directly into the kidney tissue itself, a condition called nephrocalcinosis. Over time, or with severe acute toxicity, you end up with reduced kidney function or even permanent scarring.
On the flip side, if you have chronic kidney disease (CKD), your kidneys cannot activate vitamin D efficiently. So you can become deficient in active vitamin D even if your storage levels look “normal.” That’s why people with advanced CKD often need a special prescription form of active vitamin D — not the stuff on the drugstore shelf. It’s a completely different conversation, one that requires a nephrologist.
Early Signs That Vitamin D Might Be Hurting Your Kidneys
The symptoms creep up. You might write them off as getting older, stress, or a stomach bug. In Eleanor’s case, the red flags were nausea, vomiting, poor appetite, bone pain, muscle weakness, excessive thirst, frequent urination, and confusion. You might also notice heart palpitations, high blood pressure that’s suddenly harder to control, or even depression and anxiety that doesn’t respond to usual treatment. Sometimes, it starts with a kidney stone — sudden, excruciating flank pain, blood in the urine.
Mild hypercalcemia might have no symptoms at all, which is why I can’t stress enough: if you’re taking more than the recommended dietary allowance of vitamin D, your blood work must be monitored. Symptoms usually appear when calcium climbs above 12 mg/dL, and they become an emergency above 14 mg/dL.
How We Accurately Diagnose the Problem
When I suspect vitamin D toxicity with kidney involvement, I don’t guess. I test.
The first step is a set of labs: serum calcium, albumin, creatinine (with eGFR), 25‑hydroxyvitamin D, and intact parathyroid hormone (PTH). The PTH matters because if it’s low, that tells me the hypercalcemia isn’t coming from an overactive parathyroid gland — it points squarely at the vitamin D. I’ll often add a 1,25‑dihydroxyvitamin D level if I’m dealing with a complex case, like possible granulomatous disease (sarcoidosis, tuberculosis) where inflammatory cells can activate vitamin D outside the kidneys. A 24‑hour urine calcium collection helps me see just how much calcium the kidneys are dumping and assesses the risk of stones.
An electrocardiogram (EKG) is non‑negotiable when calcium is significantly elevated; severe hypercalcemia can shorten the QT interval and cause life‑threatening arrhythmias. A renal ultrasound might follow if I see a persistent creatinine bump or calcium deposits on imaging.
The key timing: Test before you start high‑dose supplements (more than 2,000 IU daily), three to six months after you begin, and at least yearly if you stay on them. For anyone with known kidney disease, the testing interval should be even tighter, and the target vitamin D levels are individualized by a specialist.
The Most Effective Treatments — Precise Names, Dosages, and the Nuanced Context
When Eleanor’s labs came back, treatment started immediately.
Stop the source. The very first step, always, is discontinuing all vitamin D and calcium supplements. This sounds obvious, but you’d be surprised how many people hesitate. There’s no tapering needed; we just stop.
Aggressive hydration. Eleanor was markedly dehydrated. I admitted her for intravenous normal saline. The standard is 200–300 mL per hour, adjusted for her cardiac status, to push the kidneys to flush out calcium. We monitor fluid balance carefully because older patients can tip into fluid overload very quickly. A loop diuretic like furosemide (Lasix) — often 20–40 mg IV — is sometimes added only after the patient is fully rehydrated, to further block calcium reabsorption in the kidney. You never give furosemide to a dehydrated patient with hypercalcemia; it can worsen kidney injury.
Calcitonin. For a calcium level like Eleanor’s — symptomatic and above 12 mg/dL — I ordered calcitonin-salmon, 4 International Units per kilogram subcutaneously every 12 hours. Calcitonin works within hours, lowering calcium by inhibiting bone breakdown and increasing kidney calcium excretion. Its effect is fast but tapers off in a couple of days (tachyphylaxis), so it buys us time.
Bisphosphonates. The real workhorse for moderate to severe cases is an intravenous bisphosphonate. I used zoledronic acid 4 mg IV over 15 minutes once she was well hydrated and her creatinine stabilized. It potently blocks bone resorption and brings the calcium down over two to four days, with effects lasting weeks. Important caveat: zoledronic acid is contraindicated if the patient has an estimated GFR below 35 mL/min due to risk of further kidney damage and acute tubular necrosis. In patients with severe renal impairment, we might use a reduced dose of pamidronate (30–60 mg IV over several hours) after careful nephrology consultation, or rely longer on calcitonin and hydration.
Glucocorticoids. Not for garden‑variety supplement overdose, but if I suspect a granulomatous disease is producing extra 1,25‑dihydroxyvitamin D, I’d start prednisone 20–40 mg per day to dampen that aberrant activation. That’s a highly specific use case.
Dialysis. In the most extreme scenario — calcium above 18–20 mg/dL, coma, or kidney failure unresponsive to fluids — hemodialysis with a low‑calcium bath can be life‑saving. I’ve only seen it once in my career.
For Eleanor, we stopped the supplements, hydrated her vigorously, gave calcitonin and a single zoledronic acid infusion. Her calcium was 10.2 within 48 hours. Her creatinine started a slow, grateful descent.
Gentle but Proven Home Comfort Measures (When You’re Stable)
Not everyone needs the hospital. For mild toxicity caught early — say, a calcium of 10.8 mg/dL and a vitamin D level of 90 ng/mL with normal kidney function — I treat in the outpatient setting. I tell patients:
- Stop the supplement. Just that alone can drop the vitamin D level, though it takes weeks because vitamin D is fat‑soluble and hangs around.
- Drink at least 2 to 3 liters of water a day unless you have a fluid restriction. It flushes the kidneys, dilutes the urine, and reduces stone risk.
- Avoid any added calcium — no Tums as antacids, no calcium‑fortified orange juice.
- Limit sun exposure until levels normalize.
- Move if you can. Gentle walking helps prevent the bone resorption that immobility can trigger, which further spikes calcium. Eleanor took short laps around her living room.
What to Eat When Appetite Has Vanished
When your calcium is high and nausea coats every thought of food, eating feels impossible. I told Eleanor: this isn’t the time to force large meals. The goal is small, nourishing, low‑calcium bites.
- Soups and broths: Chicken or vegetable broth that’s low in sodium, maybe a clear miso soup. They hydrate while giving a little protein.
- Oatmeal or cream of wheat made with water, not milk. You can sweeten it with a little applesauce — no calcium.
- Scrambled eggs or a soft‑boiled egg, cooked without cheese or butter, easy on the stomach.
- Bananas, melon, applesauce, pear puree — gentle on the gut, minimal calcium.
- Plain crackers or rice cakes when you can only manage a nibble.
- Avoid dairy entirely: no milk, yogurt, hard cheese. They’re loaded with calcium. Skip spinach, almonds, and sesame seeds temporarily — they’re calcium‑dense. No vitamin D‑fortified foods.
Within a few days, Eleanor was eating toast with a thin smear of peanut butter and sipping chamomile tea. The appetite comes back as the calcium drops.
A Strong, Empathetic Word on Prevention
I don’t want you to be afraid of vitamin D. It is essential. Deficiency is real, especially if you have darker skin, live in northern latitudes, or avoid the sun. But “more is better” is a dangerous myth when it comes to fat‑soluble vitamins.
Here’s my own practice advice, the same I give my family.
Before you start a supplement above the basic Daily Value (600–800 IU per day for adults, as per the Institute of Medicine), get a 25‑hydroxy vitamin D test. If your level is below 20 ng/mL, you are deficient. The typical repletion dose is 1,000–2,000 IU daily, or sometimes 50,000 IU of vitamin D2 weekly for a short course, with follow‑up labs. I rarely recommend more than 4,000 IU daily for long‑term use in healthy individuals, because that is the Tolerable Upper Intake Level set by the National Academies.
If you have chronic kidney disease, do not take large doses of over‑the‑counter vitamin D without your nephrologist’s approval. You may need an activated form like calcitriol (Rocaltrol, 0.25–0.5 mcg daily) or a vitamin D analog, which directly provides the active hormone and bypasses the failing kidney’s activation step. Taking huge doses of ordinary D3 in CKD can cause a dangerous rise in calcium and phosphorus, accelerating vascular calcification.
Please, don’t get your medical advice from social media “wellness” influencers who promote megadoses of 50,000 IU daily. I have seen permanent kidney damage from that.
Can’t‑Miss Emergency Red Flags — Seek Help Immediately
These aren’t “wait and see” symptoms. If you’re on vitamin D and experience any of the following, go to the emergency room. I based these on standard hypercalcemic crisis criteria and kidney injury warning signs.
- Confusion, extreme lethargy, or you can’t stay awake. These signal the nervous system is in trouble.
- Calcium above 14 mg/dL on a lab draw — even if you feel okay, this level can trigger fatal arrhythmias.
- No urine output for more than 8–12 hours, or very dark, cola‑colored urine.
- Severe flank pain with blood in urine — think obstructing kidney stone with possible infection.
- Intractable vomiting, where you can’t keep water down, leading to severe dehydration.
- Heart palpitations, a racing, irregular heartbeat, or fainting. The EKG can show a dangerously shortened QT interval.
- Sudden, severe abdominal pain radiating to the back — pancreatitis is a known complication of severe hypercalcemia.
If there is any doubt, call your doctor or head to the emergency department. I have never faulted a patient for coming in and being safe.
A Brief, Honest Look at Potential Long‑Term Effects
The kidney has remarkable regenerative ability, but it’s not infinite. Eleanor was lucky — her acute kidney injury largely reversed over six weeks. Her creatinine settled back to 1.0. But her ultrasound did show a few tiny bright spots of early nephrocalcinosis, a permanent scar of calcium deposits in the kidney tissue. She’ll need annual kidney function checks and must be cautious about any future vitamin D or calcium use.
In more severe or prolonged toxicity, chronic kidney disease can develop and persist. Some patients never regain full function. A history of vitamin D‑associated kidney stones often means a lifelong tendency toward stone formation, requiring ongoing hydration and dietary mindfulness. And for those with unrecognized primary hyperparathyroidism or granulomatous disease, the underlying condition must be treated — otherwise the kidneys stay at risk.
I tell every patient: Your kidneys are quiet, loyal workers. They don’t complain until they’re deeply hurt. Respect them.
Eleanor and I sat together a month after her hospital stay. She had color back in her cheeks. She brought me a list again — this time, questions about safe bone health without high‑dose supplements. We talked about weight‑bearing exercise, a modest vitamin D dose of 800 IU daily, a calcium‑rich diet instead of pills, and a repeat DEXA scan. She said, “I’ll never take another pill without asking you first.” I smiled. That’s exactly the partnership I want with all of you.
About the Author
Dr. Adam N. Khan, MD, FAAFP, is a board‑certified family physician at Austin Family Health Associates in Austin, Texas. He completed his medical degree at Baylor College of Medicine and his residency in family medicine at the University of Texas at Austin Dell Medical School. A Fellow of the American Academy of Family Physicians, Dr. Khan has practiced comprehensive primary care for over 15 years, with a clinical focus on preventive medicine, metabolic bone health, and the safe management of chronic disease. He firmly believes that grounded, evidence‑based conversation is the heart of good medicine.
Medically Reviewed By
This article was reviewed for accuracy by Dr. Adam N. Khan, MD, an infectious disease specialist at the Texas Infectious Disease Institute in Austin and a clinical assistant professor of internal medicine at Dell Medical School, University of Texas at Austin. Board‑certified in internal medicine and infectious disease, Dr. Khan completed his fellowship at Johns Hopkins University School of Medicine. His expertise includes the immunological effects of vitamin D and the complex management of disorders that intersect with mineral metabolism. He confirms that every recommendation in this piece falls within current standard of care guidelines.
References
- Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. Dietary Reference Intakes for Calcium and Vitamin D. Washington (DC): National Academies Press; 2011.
- National Institutes of Health, Office of Dietary Supplements. Vitamin D: Fact Sheet for Health Professionals. Updated August 12, 2022.
- Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357(3):266‑281.
- Vieth R. Vitamin D toxicity, policy, and science. J Bone Miner Res. 2007;22 Suppl 2:V64‑V68.
- KDIGO 2017 Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease–Mineral and Bone Disorder (CKD‑MBD). Kidney Int Suppl. 2017;7:1‑59.
- Minisola S, Pepe J, Piemonte S, Cipriani C. The diagnosis and management of hypercalcaemia. BMJ. 2015;350:h2723.
- Shane E, Irani D. Hypercalcemia: pathogenesis, clinical manifestations, differential diagnosis, and management. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. (Accessed 2024).
- Araki T, Holick MF, Alfonso BD, et al. Vitamin D intoxication with severe hypercalcemia due to manufacturing error. J Med Case Rep. 2011;5:298.
- U.S. Food and Drug Administration. FDA Drug Safety Communication: Risk of severe hypercalcemia with high doses of over‑the‑counter vitamin D. Published August 2022.
- Malabanan A, Veronikis IE, Holick MF. Redefining vitamin D insufficiency. Lancet. 1998;351(9105):807‑808.
- LeFevre ML. Screening for vitamin D deficiency in adults: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2015;162(2):133‑140.