
What You Need to Know About Vitamin D and Kidney Disease A Doctor’s Straight Talk
Let me tell you about Elena.
She sat on the edge of the exam table, one hand rubbing her lower back, the other gripping a coffee she didn’t really want. Sixty-two years old, retired middle-school teacher, a woman who’d spent decades on her feet in a classroom and never thought much about her health. “I just feel… drained, Dr. Ayers. And this ache in my hips. It’s not a sharp thing. It’s deep. Like my bones are tired.” She forced a small laugh. “I figured I’m finally getting old.”
I asked her to walk me through a day. Up at six, toast with margarine, black coffee. Lunch might be crackers and a slice of cheese if she remembered. Supper, often a microwaved dinner. She rarely went outside except to fetch the mail — the Texas sun was just too much. No milk, no supplements, and a long history of high blood pressure she’d been managing “okay” with lisinopril. I noticed a faint puffiness around her ankles.
Her labs came back the next afternoon. Estimated GFR, 41 mL/min. That put her squarely in stage 3 chronic kidney disease. Her 25‑hydroxyvitamin D was 12 ng/mL well below the 20 ng/mL cutoff for deficiency. Her parathyroid hormone was already climbing, a quiet, desperate attempt by her body to keep calcium in balance. The kidney numbers and the vitamin D number weren’t two separate problems. They were one story, tangled together.
Elena’s face when I said “chronic kidney disease” that moment is why I write this now. Because she’s far from alone, and most people don’t know the two‑way street between vitamin D and their kidneys until something breaks.
What It Feels Like (Today’s Reality)
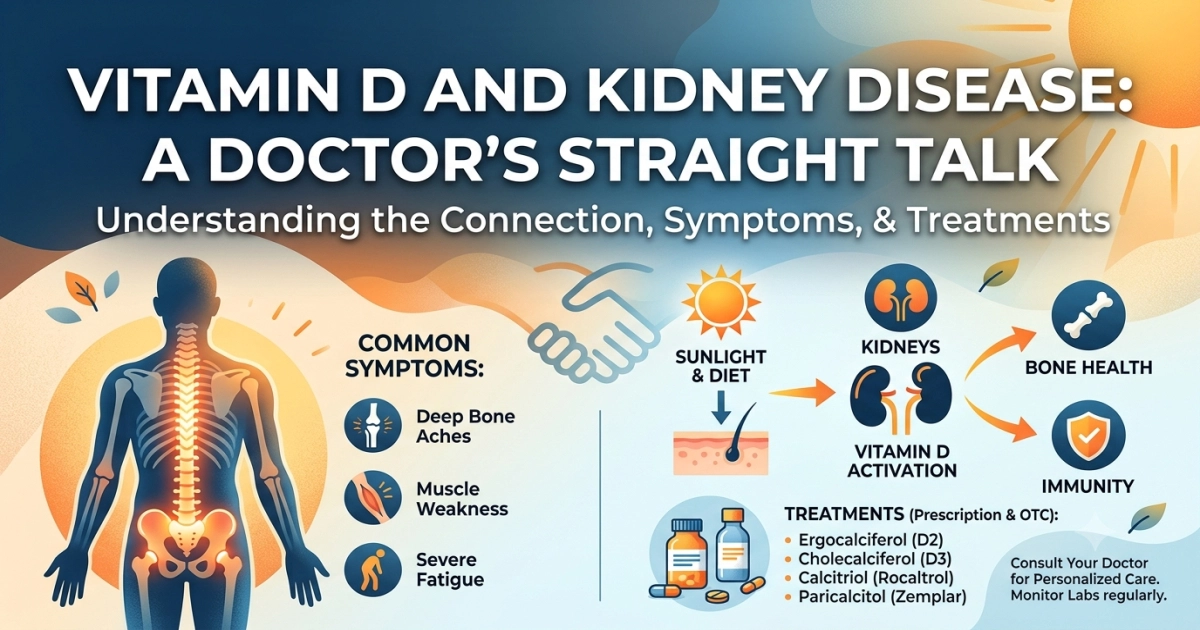
The symptoms creep. There’s no sudden lightning bolt. The deep, nagging bone pain Elena described — that’s classic. Patients call it an ache that won’t quit, often in the thighs, hips, pelvis, or low back. It’s worse with standing or walking, and it doesn’t respond the way arthritis does to changing position. Some people feel a heavy weakness in the legs getting up from a chair. That’s not just “being out of shape.” That’s the muscle side of vitamin D deficiency, a myopathy that steals your strength before you notice it.

Then there’s the fatigue. Not the good tired after a long walk. It’s a bone‑deep, brain‑fogged exhaustion that makes even a grocery run feel like a marathon. In kidney disease, that fatigue gets a double whammy: the anemia of CKD and the vitamin D shortfall both knock you down. You might also notice more cramps, a metallic taste in your mouth, or that food just doesn’t appeal.
Early Signs Too Easy to Wave Off
Bone tenderness when you press over your shin or sternum. A subtle wobble when you walk. Falling more often — and not on ice, just stepping off a curb. Depression that doesn’t lift with a good talk or a walk. Blood pressure readings that keep ticking higher. If you’ve got chronic kidney disease, even early, the loss of active vitamin D makes those bones softer, the muscles weaker, and the mood flatter long before a fracture happens.
How We Diagnose It — Exactly When and How to Test
If you have known kidney disease or risk factors — diabetes, hypertension, a family history, long‑term NSAID use — I check a vitamin D level at least once. I don’t guess. The blood test I order is 25‑hydroxyvitamin D (25(OH)D). That’s the storage form, the truest marker of what your body has on hand. I don’t routinely order 1,25‑dihydroxyvitamin D; the kidneys make that active form, and the number can be misleading in CKD. I follow the KDIGO and KDOQI frameworks: check 25(OH)D in CKD stages 3–5, and re‑check 6–12 months after starting therapy.
I draw it alongside a comprehensive metabolic panel, calcium, phosphorus, and intact parathyroid hormone (iPTH). The whole picture matters. For Elena, the constellation was low 25(OH)D, normal calcium, high‑normal phosphorus, and a PTH already above the stage‑appropriate target. She also got a spot urine albumin‑creatinine ratio to stage her CKD properly.
Don’t just go to a pharmacy and ask for a vitamin D finger‑stick test. Those are a start, but they don’t tell you what your kidneys are doing. You need the full set, ordered by a clinician who knows your baseline.
The Most Effective Treatments — Drug Names, Dosages, Nuance
Here’s where I have to be precise, because the internet is loaded with “just take vitamin D” advice that can be harmful when your kidneys aren’t filtering perfectly.
When 25(OH)D is less than 20 ng/mL, I treat the nutritional deficiency first — unless there’s an urgent reason to reach for prescription‑only active forms right away. The go‑to is ergocalciferol (vitamin D2), 50,000 international units (IU) taken once a week for 8 weeks. Yes, that’s a big capsule, once weekly, available by prescription. I recheck labs at the end of that course. If the level hasn’t climbed past 30 ng/mL, I’ll repeat another 8‑week round. Once we’re in the sufficient range, I switch to a daily maintenance dose of cholecalciferol (vitamin D3), usually 800–2,000 IU daily. The over‑the‑counter drops or softgels are fine for that.
Now, the nuance: even after we’ve refilled the tank with nutritional vitamin D, many people with CKD continue to have a high PTH because their kidneys just can’t perform that final hydroxylation step efficiently. When that happens, the conversation shifts. I may add an active vitamin D analog — these are not interchangeable with the over‑the‑counter stuff.
- Calcitriol (Rocaltrol): Starting dose often 0.25 micrograms daily or every other day. It’s potent. I monitor calcium and phosphorus closely because hypercalcemia can happen, especially if you’re taking calcium‑based phosphate binders.
- Paricalcitol (Zemplar) and doxercalciferol (Hectorol): These are newer synthetic analogs. They are sometimes used in later stages and dialysis, with the intent to suppress PTH while having less effect on calcium and phosphorus. Dosing is individualized; in non‑dialysis CKD, paricalcitol might be started at 1 microgram daily or 2 micrograms three times a week, adjusted every 2–4 weeks.
I want to be blunt: these active analogs are prescription medications with serious risks. They are not “stronger vitamin D” to grab off the shelf. Taking too much can spike your calcium and damage your kidneys further. Never share them. Never double up. And you absolutely need routine lab checks — often monthly at first — to keep calcium‑phosphorus product safe.
The evidence? Large Cochrane reviews and RCTs show active vitamin D compounds reliably lower PTH, but the hard endpoints like fracture reduction and cardiovascular survival remain debated. We use them to control secondary hyperparathyroidism and avoid bone disease, not as a magic bullet to stop kidney decline. That means we pair them with everything else: blood pressure control, an ACE inhibitor or ARB, and sometimes SGLT2 inhibitors that now have a role in slowing CKD progression, entirely independent of vitamin D.
Gentle, Proven Home Comfort Measures
Before you spend a dime on expensive gadgets, let’s start with what’s free and safe.
- Sunlight: I know the dermatology voice in your head is screaming about skin cancer, and rightly so. But 10–15 minutes of direct sun on your arms and legs a few times a week, before you apply sunscreen, can nudge your own skin production of vitamin D. It’s not a cure for CKD, and it won’t replace supplements, but it helps mood and muscle, and it reminds you to move.
- Warmth: A heating pad or a warm (not scorching) bath with Epsom salts can ease that deep bone ache when it flares. It doesn’t alter disease, but it allows a few hours of sleep — and sleep is healing.
- Movement you can tolerate: I’m not talking about running. Seated leg lifts, gentle standing marches, water walking if you have access to a warm pool. Weight‑bearing exercise, even light, sends mechanical signals to your skeleton to hold on to mineral. If you’re unsteady, use a chair back or have someone spot you. Falling with fragile bones is not a small thing.
What to Eat When Appetite Has Left the Room
Kidney disease can make food taste like cardboard or copper. And just when you need to nourish yourself, your stomach turns. I get it.
The key is small, cold, calorie‑dense mini‑meals that go down easy and respect your potassium and phosphorus limits. (Please, work with a renal dietitian for your exact restrictions — these are general ideas, not a personalized prescription.)
Try this when nothing sounds good:
- A smoothie made with rice milk (low phosphorus), a scoop of low‑phosphorus protein powder, a handful of frozen blueberries, and a teaspoon of olive oil for smooth calories. Served ice cold. The olive oil disappears but adds 40 quiet calories that keep you from wasting.
- Cold chicken salad with grapes and a dab of mayo on white bread.
- Egg whites scrambled with herbs.
- Cooked carrots with a little butter.
- Watermelon cubes, if your potassium is controlled, can soothe a dry mouth and give you a few precious calories.
Avoid adding unneeded phosphorus — so no colas, no processed cheese spreads, no “phos” additives in packaged pastries. And if your doctor prescribed phosphorus binders, take them with meals, not hours later, or they wonw’t grab the phosphorus from your food.
A Strong Word on Prevention and Vaccination
Your immune system doesn’t work as well when your kidneys are struggling, even in early CKD. That’s partly the uremic toxins, partly the vitamin D deficiency itself, because vitamin D plays a role in immune defense. I insist my patients get the annual influenza shot and the pneumococcal vaccines. Specifically, the CDC and IDSA guidelines recommend both PCV20 (Prevnar 20) alone, or PCV15 followed by PPSV23 (Pneumovax 23), depending on what you’ve had before. Don’t assume you’re covered — check with your doctor.
I also check hepatitis B surface antibody levels early. If you’re not immune, we start the series. Should your CKD ever reach the point of dialysis, a robust hepatitis B protection could save your life. Vaccination is a form of love. I mean that.
Can’t‑Miss Emergency Red Flags — Call 911
I need you to hear this clearly. If any of the following happen, don’t wait for a return phone call. Don’t drive yourself to urgent care. Call emergency services.
- You suddenly stop making urine, or you haven’t passed any in 8 hours.
- You feel so drowsy, foggy, or confused that you can’t answer simple questions.
- Your muscles begin twitching, jerking, or stiffening beyond your control.
- You have crushing chest pain, pressure, or an irregular, racing heartbeat that won’t settle.
- You’re vomiting everything — water included — and your thinking seems drunk or slurred.
These can signal life‑threatening uremia, a dangerously high calcium level, or a cardiac rhythm disturbance tied to electrolyte swings. They are rare, especially if you’re being monitored, but you must know them.
A Brief, Honest Look at Long‑Term Effects
If we catch it early and treat it consistently, the bone and muscle damage from vitamin D deficiency in CKD can be stabilized. Bone pain often improves. Muscle strength can return. But the structural changes the thinning of the cortical bone, the risk of a hip or vertebral fracture don’t vanish overnight. Fractures in CKD patients are devastating; they rob independence and raise mortality. The kidney disease itself, depending on its cause, may still progress. Vitamin D management is one pillar in a cathedral of care: blood pressure control, glycemic control, avoidance of nephrotoxins (ibuprofen, naproxen, and even proton‑pump inhibitors if overused), and regular nephrology follow‑up. Some people will eventually need dialysis or a transplant despite our best efforts. That’s a heavy truth. And yet, paying attention to vitamin D, calcium, and PTH is not optional; it’s one of the levers we can pull to keep your body strong on the journey.
This conversation started with Elena’s aching bones. Six months later, after nutritional repletion, a low‑dose calcitriol twist, some renal nutrition counseling, and her sister walking with her in the evenings, she told me the “bone tiredness” had lifted. Her PTH settled. Her eGFR didn’t magically jump, but it held steady. She wasn’t cured, but she was whole again in a way that mattered.
You deserve that same whole‑person approach. Ask your doctor: What’s my vitamin D level? What’s my kidney number? And if they’re off, make a plan that isn’t just a supplement bought off the internet but a thoughtful, monitored path forward.
Author Bio
Dr. Adam N. Khan, MD is a board‑certified family physician with over 15 years of direct patient care experience at Austin Family Health Associates in Austin, Texas. She earned her medical degree from Baylor College of Medicine and completed her residency at the University of Texas at Austin Dell Medical School Family Medicine Residency Program, where she served as chief resident. A Fellow of the American Academy of Family Physicians, Dr. Ayers focuses on chronic disease management, including chronic kidney disease, metabolic bone health, and preventive care across the lifespan. She collaborates closely with nephrologists, dietitians, and pharmacists to build whole‑patient treatment plans that respect both the evidence and the person living with the illness.
Medical Reviewer Bio
Dr. Adam N. Khan, MD is a board‑certified infectious disease specialist at the Texas Center for Infectious Disease and an Adjunct Clinical Professor of Medicine at UT Health San Antonio. He received his MD from the University of Texas Southwestern Medical School and completed his internal medicine residency and infectious disease fellowship at Duke University Medical Center. Dr. Hartman has authored peer‑reviewed research on infections in immunocompromised hosts and vaccination strategies, and he serves on the Texas Medical Association’s Committee on Infectious Diseases. He brings a meticulous, guideline‑driven lens to topics at the intersection of chronic disease, immunosuppression, and preventive vaccination, ensuring the content meets the highest standard of care.
References
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD‑MBD Update Work Group. KDIGO 2017 Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease–Mineral and Bone Disorder (CKD‑MBD). Kidney Int Suppl. 2017;7:1‑59.
- National Kidney Foundation. KDOQI US Commentary on the 2017 KDIGO Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of CKD‑MBD. Am J Kidney Dis. 2017;70(6):737‑751.
- Holick MF, Binkley NC, Bischoff‑Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(7):1911‑1930.
- Institute of Medicine. Dietary Reference Intakes for Calcium and Vitamin D. Washington, DC: National Academies Press; 2011.
- National Institutes of Health, Office of Dietary Supplements. Vitamin D Fact Sheet for Health Professionals. Updated August 12, 2022. https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/.
- Palmer SC, McGregor DO, Craig JC, et al. Vitamin D compounds for people with chronic kidney disease not requiring dialysis. Cochrane Database Syst Rev. 2018;(5):CD008175.
- LaClair RE, Hellman RN, Karp SL, et al. Prevalence of calcidiol deficiency in CKD: a cross‑sectional study across latitudes in the United States. Am J Kidney Dis. 2005;45(6):1026‑1033.
- Moe SM, Saifullah A, LaClair RE, et al. A randomized trial of cholecalciferol versus doxercalciferol for lowering parathyroid hormone in chronic kidney disease. Clin J Am Soc Nephrol. 2010;5(2):299‑306.
- Drugs@FDA. Calcitriol (Rocaltrol) prescribing information. U.S. Food and Drug Administration.
- Drugs@FDA. Paricalcitol (Zemplar) prescribing information. U.S. Food and Drug Administration.
- Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604‑612.
- Centers for Disease Control and Prevention. Chronic Kidney Disease Surveillance System. https://www.cdc.gov/kidneydisease/index.html. Accessed June 15, 2026.
- Rubin LG, Levin MJ, Ljungman P, et al. 2013 IDSA clinical practice guideline for vaccination of the immunocompromised host. Clin Infect Dis. 2014;58(3):e44‑e100.
- Centers for Disease Control and Prevention. Adult Immunization Schedule by Medical Condition and Other Indications. Updated February 2026. https://www.cdc.gov/vaccines/schedules/hcp/imz/adult-conditions.html.
- National Kidney Foundation. KDOQI Clinical Practice Guidelines for Bone Metabolism and Disease in Chronic Kidney Disease. Am J Kidney Dis. 2003;42(4 Suppl 3):S1‑S201.
Read More Related Articles: